
 Pain. When I was in residency they called it the 5th vital sign. The quantification of pain was as necessary and as important as a patient’s blood pressure, heart rate, respiratory rate and temperature. Assess their pain. Relieve their pain. Make it go away.
Pain. When I was in residency they called it the 5th vital sign. The quantification of pain was as necessary and as important as a patient’s blood pressure, heart rate, respiratory rate and temperature. Assess their pain. Relieve their pain. Make it go away.
Pain (like death) is the enemy of every good doctor and to really do your job, to be a good doctor, you must eliminate the pain. It seemed like a good idea at the time. The patients certainly liked it. It made the doctors’ and nurses’ jobs easier. Pain-free patients meant quiet and comfortable patients. They weren’t writhing. They weren’t screaming.
This same concept spilled over into the outpatient setting.
Pain can not be measured by a particular test or scan. It can only be expressed by patients. A tool has been developed to help quantify pain. You may have seen it before. It kind of looks like a series of pre-emoji faces.
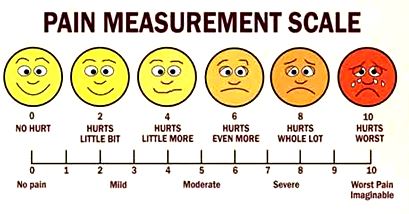 What is your pain level? On a scale from 1-10, where are you today? Point at the series of faces that go from smiling to barfing in agony, which one most represents your level of pain?
What is your pain level? On a scale from 1-10, where are you today? Point at the series of faces that go from smiling to barfing in agony, which one most represents your level of pain?
Inevitably, the woman who walked in of her own accord, hair in place, make-up just so, even a few bangle bracelets on her arm as if she put some thought into her appearance, would answer, “I’m a 13 on the pain scale and I’m that face with the knife sticking in its eye,” smile.
OK. Let me explain. A 13 is when you are lying on a train track and a train just ran over your legs. One leg is barely attached and the other one is still stuck on the front of the train. Are you still a 13?
No. Now I’m a 15.
And that’s how the prescription drug problem began. Doctors are human, that I can attest to. Doctors have empathy. We don’t like to see others in pain. If a patient says that they are a 15 on a pain scale that only goes to 10, well, gosh that’s terrible and I, being the great doctor that I am, will fix it. And be the hero. And save the day. And fuel an addiction.
Do people really have that kind of pain? Um, yes. Do people really need prescription pain medications? Um, yes. Do people who don’t really need prescription pain medications find ways to get them because they really like the way these drugs make them feel? Um, unfortunately, yes.
So how does a doctor, human and empathetic, give the right people the right meds to help with their pain and not become a glorified drug dealer? How does a doctor not continue to perpetuate a system that has resulted in 40 Americans dying every day from prescription pain medications? There are more deaths from prescription narcotic overdoses than any other drug, legal or illegal. Didn’t doctors take an oath to first do no harm? I did.
In March 2016, the CDC published the CDC Guideline for Prescribing Opioids for Chronic Pain which is an attempt to help doctors treat chronic pain without harming their patients. The guidelines are directed at primary care physicians, who prescribe about half of all pain medications in the US. The CDC offers a common sense approach to prescribing medications for pain:
- Use non-narcotic medications, such as anti-inflammatories to treat pain
- When necessary, use the lowest dose narcotic to bring relief
- Use the narcotic for the least amount of time possible, especially for acute pain -about 3 days
- Prescribe only the amount of pills necessary
- Use shorter acting narcotics
- Follow up and reevaluate patients frequently -about every 3 months
- Use other modalities to treat pain: cognitive, behavioral, physical therapy
- Avoid prescribing opiates and benzodiazepines together
- Utilize urine drug screens to assess for use of medication and/or other illicit substances
- Assess the patient’s history of addiction to evaluate risk
- Have a treatment plan in place, discuss risks of narcotic medications with patients
- Discuss treatment options if a patient becomes addicted (methadone or buprenorphone)
It’s a start. It’s a direction. It’s a lifeline. There is no doubt that prescription pain medications have caused an epidemic of addiction, overdose, and death in this country. Doctors are the gatekeepers of these dangerous drugs. Drugs that in the right person, for the right affliction, can bring relief, but can be equally deadly. It is up to doctors to yield the power of their pen to write prescription narcotics carefully and conservatively. It is up to doctors to understand the danger that lurks in the very medication that they were once encouraged and expected to use in patients to alleviate their pain.
http://www.cdc.gov/drugoverdose/prescribing/guideline.html




Thank you for this! My daughter was a heroin addict. I certainly don’t blame doctors for her problem, but many of my patients on the ambulance were addicted to prescription medications and moved on from there. Some died. Her first bad OD was from Fentanyl! At 19! Where did she get that I always wondered. It’s nuts. It the small state of NH it’s epidemic proportions. They are now dispensing Narcan to families to save their own people because we couldn’t get there fast enough. Some are against it, but I say: hey, if it buys us time in the ambulance, go for it! Who am I to say don’t give something like that to a mother standing over her kid who isn’t breathing??? But again, you write a humble and poignant piece about this subject. Thank you again. And oh, BTW, my daughter is doing great now.
LikeLike
I’m so glad your daughter is doing well! This is a horrible epidemic and docs aren’t talking about it. It’s hard -we want to help people, but even the best of us have been snowed by a patient. These drugs are so addictive and dangerous. Personally I tend to refer patients to pain clinics but it doesn’t make the problem go away I just don’t have to see it or be a part of it. I don’t know what the answer is. We were taught and encouraged to use these drugs in patients with little fear and that was wrong.
LikeLiked by 1 person
We all just do the best we can.
LikeLiked by 1 person
What is that saying? The road to hell is paved with good intentions…
LikeLiked by 1 person